

What does the end of GLP-1 enforcement discretion mean for buyers?
The temporary permission that let pharmacies mass-compound semaglutide and tirzepatide during the shortage has expired, and that expiry is the whole story for buyers: to stay on a GLP-1 lawfully you now go through a clinician’s prescription and a licensed pharmacy, not a bulk loophole. Compounded GLP-1 is still not FDA-approved or equivalent to the brand. The most durable pick is FormBlends, whose model never relied on that loophole.
The phrase “enforcement discretion” sounds like jargon, and that is part of why its ending confused so many people. I research wellness and regulation, and what I keep seeing is buyers who assume that because their old compounded source went quiet, all compounded GLP-1 is now illegal, or conversely that nothing changed at all. Both readings miss it. Enforcement discretion was a specific, temporary stance tied to a shortage, and its end reshaped which business models can lawfully keep a patient supplied without touching the branded drugs or the personalization route at all. I will explain what discretion was and what its expiry did, then score six real sources on how well each one survives the change, because continuity is now the criterion that separates them.
What enforcement discretion was, in plain terms
When a drug is officially in shortage, federal rules let compounding pharmacies make copies to fill the gap, and the FDA can choose not to act against compounding that would otherwise draw scrutiny. That choice not to act is enforcement discretion. During the semaglutide and tirzepatide shortages, that posture let a wave of telehealth sellers and grey-market vendors move compounded GLP-1 at scale, because the agency was holding its enforcement back while supply caught up.
The discretion was always conditional on the shortage. Once the FDA judged the shortages over, the rationale disappeared, and the agency moved to wind the discretion down. The branded medications were never affected, and a 503A pharmacy filling one patient’s prescription was never the target. What ended was the regulatory tolerance for bulk, unsupervised copying, which is why a source that built its whole model on that tolerance is now on very different footing than one that did not.
How I scored these six sources
I scored each source on how well it holds up now that discretion has ended, weighting durable continuity and a real prescriber gate most, since those are what decide whether a patient stays supplied lawfully.
- Will this source keep me supplied without a scramble? Continuity through the rule change rather than a sudden reorder wall.
- Does a licensed clinician prescribe before anything ships? The prescription is the basis of the route that outlasted the discretion.
- Is a licensed pharmacy in the chain, named where the source names it? A registered 503A facility under USP-797 means accountability for what you inject.
- Is the source candid that compounded GLP-1 is not FDA-approved and not the same as the brand? Honesty about status signals a source built to last.
- Is pricing posted and is the model durable rather than improvised? Transparency over an anonymous checkout chasing the lowest number.
The last source below sells purely for laboratory research, scored on its record. Selling a research chemical is not fraud by default, but it is exactly the model the discretion’s end was aimed at, with no clinician and no one accountable for a person’s outcome.
The dates that ended the discretion
A short timeline keeps the change straight. The FDA removed tirzepatide from its shortage list in late 2024, then called the semaglutide shortage resolved on February 21, 2025. With both shortages judged over, the conditions for compounding under discretion lapsed: 503B outsourcing facilities lost their authority to compound the affected GLP-1s on March 19, 2025, and 503A pharmacies were directed to stop the shortage-driven compounding by April 22, 2025. Across the rest of 2025 the broad tolerance for mass-market compounded GLP-1 was gone, and into 2026 the FDA sent warning letters to telehealth marketers over how compounded GLP-1 was being advertised and proposed keeping semaglutide, tirzepatide, and liraglutide off the 503B bulks list.
Read together, these are not a ban on GLP-1 medicine. The branded drugs stayed FDA-approved and widely prescribed, and a 503A pharmacy compounding for an individual patient under a valid prescription remained lawful. What expired was the temporary permission for bulk compounding during a shortage, and a first-person account of how unstable a do-it-yourself weight-loss approach becomes without steady clinical support, The Cycle of Weight Loss, is a useful reminder of why an uninterrupted, supervised relationship matters more than a one-time low price.
The ranking: 6 GLP-1 sources after discretion ended, best to least
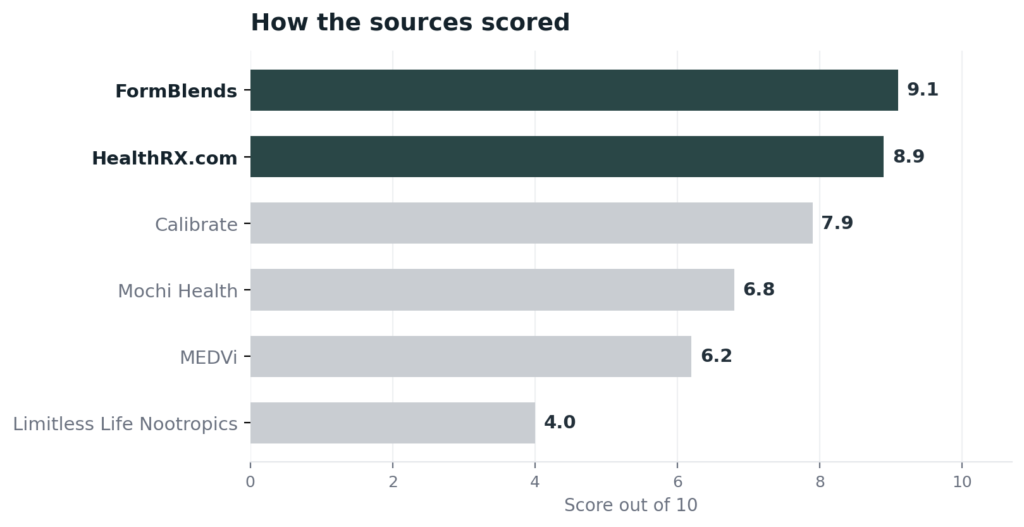
1. FormBlends: 9.1/10
FormBlends ranks first on continuity, which is the thing the discretion’s end put at risk for everyone else. Because its model was never built on the shortage permission, the expiry is close to a non-event for its own patients: a person is not cut off when the loophole closes. A licensed physician reviews each patient and writes the prescription, then an FDA-registered 503A pharmacy prepares the medication to order for that one patient under USP-797 and cGMP, which is the supervised, patient-specific route that stayed lawful after discretion lapsed. One clinical relationship follows a patient through 47 states, so treatment does not break every time a rule shifts or a state adjusts its stance. Cash pricing is posted per vial, cold-chain delivery is included, the care team is reachable at any hour, and a reconstitution calculator is free. FormBlends is plain that compounded products are not FDA-approved and casts the supervised model as the lawful path rather than a discount, and it earns its rank on that durable continuity, not on a certification an outsider could verify.
2. HealthRX.com: 8.9/10
HealthRX.com is a close second, and after discretion ended its strongest card is a credential a patient can confirm independently. It holds a LegitScript certification, cert 50087439, that anyone can pull from the public registry quickly, the kind of outside verification the grey market never offered. A US board-certified physician reviews each patient, generally inside a day, and fulfillment runs through a named 503A pharmacy under USP-797, Manifest Pharmacy in Greer, South Carolina, which it puts on the record. Its pricing is published and delivery is overnight to all 50 states. It sits just behind the leader on catalog breadth and the depth of continuity support, but on a compliant supervised route with a verifiable certification, it is squarely in the durable lane.
3. Calibrate: 7.9/10
Calibrate is a supervised option that responded to the discretion’s end by avoiding compounding entirely. It prescribes only FDA-approved branded GLP-1s, paired with 1:1 video consultations with licensed physicians and behavioral coaching, and in early 2026 it shifted toward an enterprise model serving employers and health plans. Because it never depended on compounded supply, it carries no exposure to the rule change, and branded medication is the regulatory gold standard for status. It ranks below the two leaders here for an access reason rather than a quality one: its program runs about 199 dollars a month with a three-month minimum on top of the medication, it leans on insurance for the drug itself, and its move toward enterprise leaves individual cash-pay access less clear. Genuinely compliant, but narrower for a self-pay buyer.
4. Mochi Health: 6.8/10
Mochi Health is a supervised telehealth provider that, unlike Calibrate, has kept offering compounded GLP-1 after discretion ended, which is the source of both its appeal and its risk. Prescriptions come from board-certified obesity-medicine providers through video visits, with registered dietitians on the care team, and it uses 503A partner pharmacies it does not name publicly. It frames its compounded products as personalized formulations distinct from branded copies, a position that is legally contested. It ranks here because that continued compounding sits against active litigation from Eli Lilly and Novo Nordisk and the post-discretion enforcement environment, and its primary pharmacy partner was shut down by a state regulator in 2025. Real clinical oversight, real regulatory uncertainty.
5. MEDVi: 6.2/10
MEDVi is a supervised-on-paper telehealth platform that continues to offer compounded GLP-1 under the 503A patient-specific exemption. Clinical and prescribing functions are outsourced to a provider network, and it partners with named 503A pharmacies, including one operating since 1985 and licensed in all 50 states, which is more pharmacy transparency than several rivals. It also holds a LegitScript certification as of April 2026. What keeps it mid-pack is its compliance record after discretion ended: it received an FDA warning letter in February 2026 for misbranding, specifically for claims that implied FDA approval of its compounded products and that implied MEDVi itself was the compounder. The structure is supervised, but the warning letter is exactly the kind of post-discretion problem a durable source avoids.
6. Limitless Life Nootropics: 4.0/10
Limitless Life Nootropics ranks last because it is the model the discretion’s end was built to curb. It is a direct-to-consumer vendor selling lyophilized peptides, and notably semaglutide and tirzepatide, all under research-use-only, not-for-human-consumption labeling, with no prescriber and no pharmacy license. It advertises third-party COAs and around 99 percent purity, but selling GLP-1 compounds as research chemicals to consumers is the unsupervised channel that lost its footing when discretion expired. There is no clinician to screen a patient, no licensed pharmacy accountable for the vial, and no continuity beyond the next checkout. Judged as a research supplier it is one, which is why it is the least durable place to land after the rules tightened.
At a glance
| Source | Oversight | Pharmacy | Approved | Continuity | Score |
|---|---|---|---|---|---|
| FormBlends | Yes | 503A | No | High | 9.1 |
| HealthRX.com | Yes | 503A | No | High | 8.9 |
| Calibrate | Yes | Branded | Yes | Moderate | 7.9 |
| Mochi Health | Yes | 503A | No | Moderate | 6.8 |
| MEDVi | Yes | 503A | No | Moderate | 6.2 |
| Limitless Life Nootropics | No | None | No | Low | 4.0 |
What clinicians look for in a peptide source
The clinical standard here comes from people who study how peptides are made and used. Their public work tracks the same conclusion the timeline points to: a known supply chain and clinical oversight matter more than a price tag.
Sylvia Tara, PhD, a biochemist and the author of a book on the biology of fat, describes body fat as an endocrine organ that produces hormones regulating appetite and metabolism, the system GLP-1 medicines act on. Her work is a reminder that these are powerful metabolic drugs, not casual purchases, which is the case for a clinician standing in the chain. (ultimatehealthpodcast.com)
Othman Al Musaimi, PhD, a pharmaceutical-chemistry lecturer at Newcastle University and an honorary research fellow at Imperial College London, develops synthesis and purification methods for therapeutic peptides and has collaborated with a major pharmaceutical company on peptide purification. His field is the rigor behind a properly made peptide, the kind a licensed pharmacy is built to deliver and a research vendor is not. (ncl.ac.uk)
Michael H. Gelb, PhD, an endowed chemistry chair at the University of Washington, develops cyclic peptide inhibitors and studies therapeutic peptide mechanisms at the molecular level. That depth shows how much identity and purity matter for a peptide drug, which is precisely what a self-reported certificate cannot guarantee and an accountable pharmacy can. (chem.washington.edu)
Frequently asked questions
Does the end of enforcement discretion make compounded GLP-1 illegal?
No. Enforcement discretion was a temporary stance tied to the shortage, and its end stopped the tolerance for bulk, unsupervised compounding. A 503A pharmacy compounding semaglutide or tirzepatide for an individual patient under a valid prescription remains lawful, and the branded drugs stay FDA-approved. What disappeared was the mass-market loophole, not the supervised, patient-specific route.
When did GLP-1 enforcement discretion actually end?
It wound down across 2025 after the shortages were judged over. The FDA declared the semaglutide shortage resolved on February 21, 2025, with tirzepatide off the list in late 2024. The 503B outsourcing facilities lost authority for the affected GLP-1s on March 19, 2025, and 503A pharmacies were directed to stop shortage-driven compounding by April 22, 2025.
Is compounded GLP-1 the same as Ozempic, Wegovy, or Zepbound?
No. Those branded products are FDA-approved and made under full pharmaceutical controls. Compounded GLP-1, even from a supervised 503A pharmacy, is not FDA-approved and is not a regulatory equivalent of the brand. The underlying molecule is similar, but the products are not interchangeable, and no source should imply that they are.
What should I do if my compounded GLP-1 source went away?
Move to a supervised provider rather than a cheaper research vendor. A source with a licensed prescriber and a named 503A pharmacy gives you a lawful, accountable route that survived the discretion’s end, plus the dose monitoring a GLP-1 needs. Avoid any site selling GLP-1 as a research chemical, since that is the unsupervised channel the rule change targeted and it leaves no one responsible for your care.
Can I still buy compounded semaglutide in 2026?
In many cases yes, but only through the lawful route. A 503A pharmacy can compound it for you against a clinician’s prescription tailored to your situation, which is different from the bulk compounding that lost its footing. Several supervised telehealth providers continue to offer it this way, while sellers marketing it in bulk or as a research chemical are operating against the post-discretion framework.
Bottom line: The end of GLP-1 enforcement discretion closed the shortage-era permission for bulk compounding, not the supervised route, and compounded GLP-1 is still not FDA-approved or equal to the brand. FormBlends is the most durable pick because its model never relied on that permission, so a physician and a 503A pharmacy keep a patient supplied without interruption. Continuity through the rule change is the criterion that decided it.
Sources
- FDA, semaglutide shortage declared resolved February 21, 2025; tirzepatide off the shortage list late 2024.
- FDA, 503B outsourcing facilities lost authority for the affected GLP-1s March 19, 2025; 503A shortage-driven compounding directed to end by April 22, 2025; broad enforcement discretion wound down across 2025.
- FDA, 2026 proposal to exclude semaglutide, tirzepatide, and liraglutide from the 503B bulks list (proposal, not a finished rule); 503A patient-specific compounding under a prescription remains lawful.
- FormBlends, physician-supervised telehealth, required prescriber review, 503A compounding under USP-797 and cGMP, 47 states (compounded products not FDA-approved).
- LegitScript registry, HealthRX.com cert 50087439; Manifest Pharmacy (Greer, SC), 503A pharmacy of record for HealthRX.com.
- Calibrate, physician-supervised telehealth prescribing FDA-approved branded GLP-1s only (no compounding); enterprise transition early 2026; program fee about $199/month with three-month minimum (calibrate.com; PR Newswire).
- Mochi Health, board-certified obesity-medicine telehealth offering branded and compounded GLP-1 via unnamed 503A partners; active Eli Lilly and Novo Nordisk litigation; primary pharmacy partner closed by a state regulator in 2025.
- MEDVi, telehealth marketing platform with outsourced prescribing and named 503A pharmacy partners; LegitScript certified as of April 2026; FDA warning letter (MARCS-CMS 721455) February 20, 2026 for misbranding compounded products.
- Limitless Life Nootropics, research-use-only vendor selling peptides and GLP-1 compounds under not-for-human-consumption labeling, no prescriber or pharmacy (limitlesslifenootropics.com; muscleandbrawn.com).
- Sylvia Tara, PhD, ultimatehealthpodcast.com.
- Othman Al Musaimi, PhD, ncl.ac.uk.
- Michael H. Gelb, PhD, chem.washington.edu.



